Map the disease.
Validate the drug.
Computational Disease Analysis reports for foundations, biotech, and pharma R&D.
PHYSIM maps disease failure architecture down to the cell, identifies structurally critical targets, and validates candidate engagement through a 7-gate deterministic gauntlet. No AI guessing. No confidence scores. Same molecule, same answer, every time.
6,675 diseases mapped. 97.8% concordance with clinical reality. Standard screening stops at pharmacokinetics — that's Gate 1. We go to Gate 7.
The difference between guessing and measuring
Every AI drug discovery platform on the market is probabilistic — it learns from past data, then predicts what might happen next. PHYSIM doesn't predict. It computes. That's not a marketing distinction. It's a physics distinction.


When physics agrees with clinical reality
Every claim below was computed — not learned from training data, not inferred from patterns, not predicted from historical outcomes. The engine takes molecular structure as input and computes physical survival. These are the results.
Every compound class in the global pharmacological registry — approved, experimental, investigational, withdrawn, and illicit — was computed through the full 15-stage gauntlet.
Per-stage concordance — the rate at which each individual biological computation agrees with observed outcomes. 14,606 compounds × 15 stages = 219,090 evaluations.
Where disease architecture becomes drug targets.
My proprietary platform translates raw biological failure into actionable, targetable molecular blueprints. The engine maps the full structural progression of a disease — from first cellular compromise through irreversible collapse — and identifies exactly where a drug can intervene.
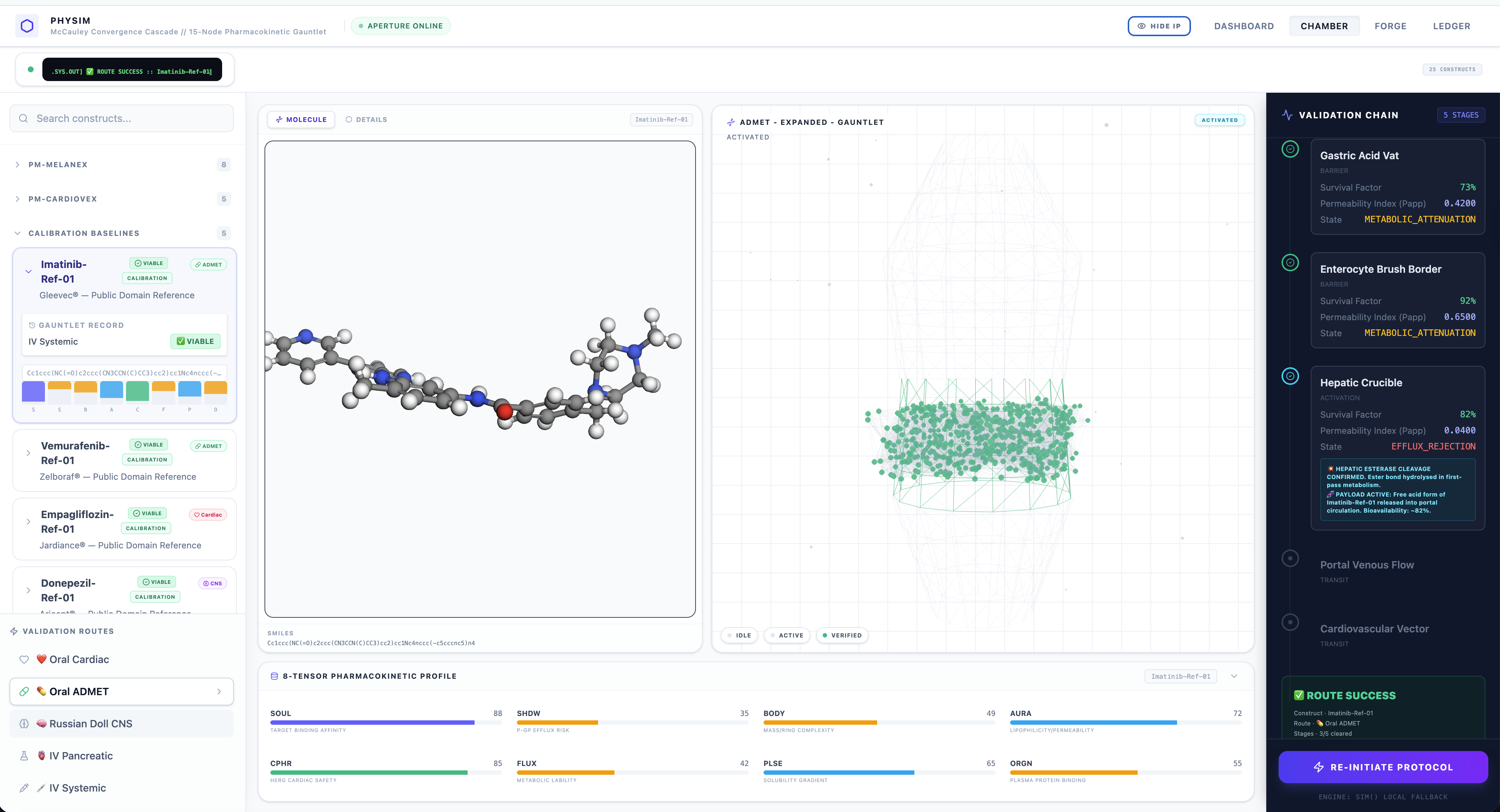
Watch a compound fight for survival.
The interactive ADMET gauntlet below demonstrates how a molecule is tested against each biological checkpoint in real time.
One deterministic engine. Four commercial outcomes.
Disease architecture, critical target computation, candidate validation, and pre-clinical reporting — computed as one structural problem.
Disease Architecture Mapping
Give us a disease. We return its structural blueprint — every pathway, every convergence point, every stage of collapse from first cellular compromise through irreversible progression. We don't read the literature. We compute the architecture. 6,675 diseases mapped and counting.
Target Acquisition & Drug Repurposing
The engine identifies which molecular structures can engage a disease — including FDA-approved drugs that may already work but have never been tested against the target. New candidates. Existing drugs. All computationally validated against the disease's actual failure architecture.
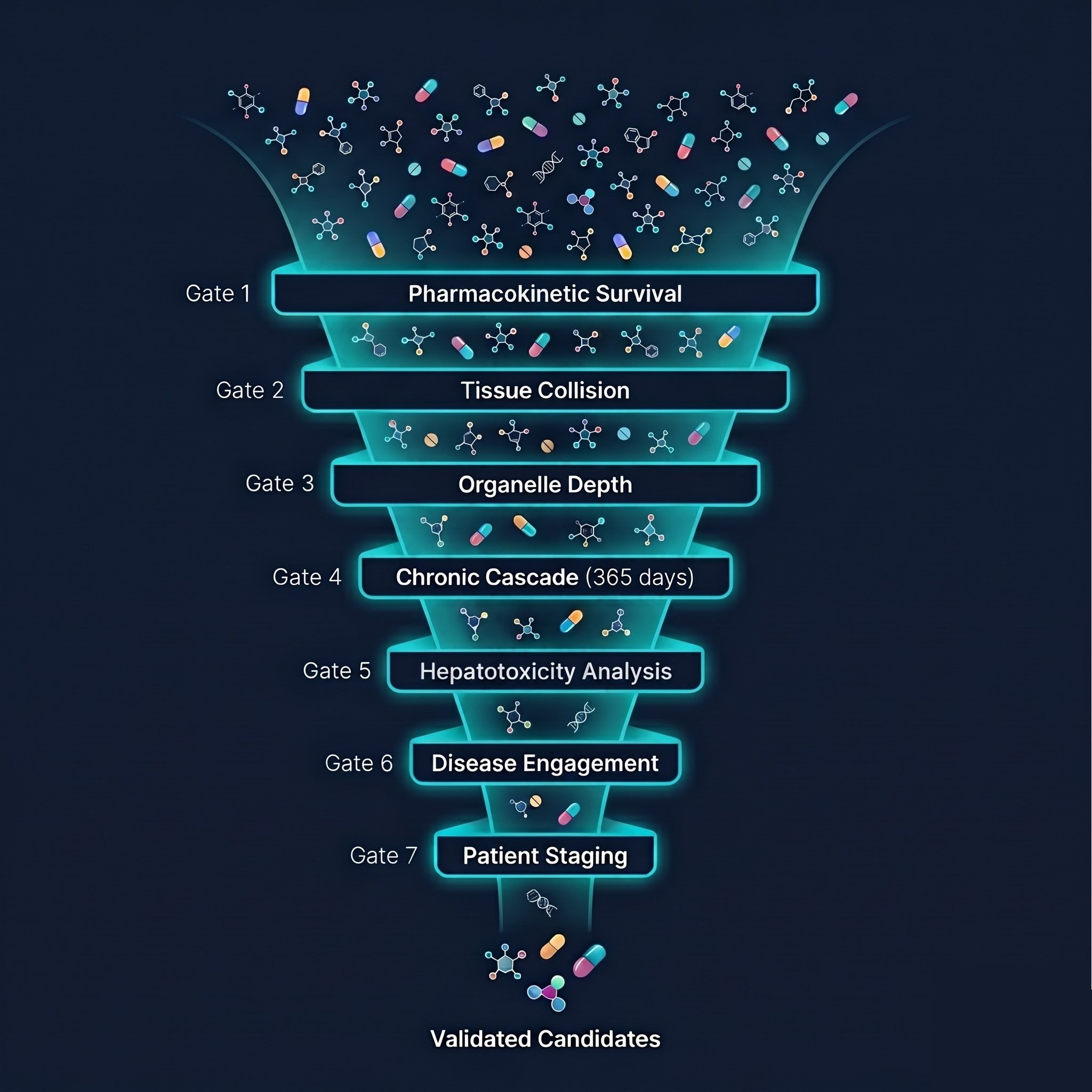
7-Gate Candidate Validation
Every candidate survives a 7-gate gauntlet — from pharmacokinetic survival through tissue penetration, organelle-depth interaction, chronic dosage safety, liver toxicity, disease engagement, and patient-stage matching. The molecule doesn't pass a checklist. It survives a computational body.
ADMET Is Gate 1. We Go to Gate 7.
Traditional tools stop at pharmacokinetics — absorption, distribution, metabolism, elimination, and toxicity. That is the first gate inside a much larger computation. PHYSIM continues through tissue penetration, organelle-depth interaction, chronic exposure, hepatotoxicity analysis, disease engagement, and patient-stage matching. ADMET is included. It is not the category.
Pre-Clinical Grade Report
You receive a complete, auditable report documenting every gate: pharmacokinetic profile, safety panel (hERG, BBB, CYP450), chronic toxicity timeline across dosage and duration, DILI proximity scoring, disease engagement mapping, and patient stage classification. Ready for your wet lab, your investors, or your regulatory filing.
Computed against clinical reality — and verified
These are not projections. Every metric was earned through 219,090 individual physical evaluations — benchmarked against known clinical outcomes across the full pharmacological registry. No model. No training data. Pure structural physics.
219,090 individual physical evaluations against 14,606 compounds. Not predictions — deterministic computations from molecular structure. Each of 15 pharmacokinetic stages was independently scored against clinical outcome data.
The Synthetic Human Chamber — a proprietary body simulation engine — correctly computes the physical survival of 97.8% of FDA-approved compounds through 15 physiological kill gates. The 2.2% gap is the frontier of approximation, not prediction error.
Every compound with a valid molecular structure in the global pharmacological registry — approved, experimental, investigational, and withdrawn — was processed through the full engine at 215 compounds per second. No model. No training data. Pure structural physics.
ADMET is a checklist. This engine simulates a body.
Standard computational screening treats each biological checkpoint as an independent pass/fail gate — a checklist. The Synthetic Human Chamber simulates continuous body traversal: a molecule enters the GI tract, survives absorption, distributes through real tissue geometry, and either reaches the target or gets killed. Compounds that traditional screening incorrectly rejects are recovered. The ones that are genuinely dangerous are caught.
Not a faster version of the old workflow. A different computational category.
Traditional pharma fragments the problem. Standard AI accelerates fragments. PHYSIM computes the full structural relationship between disease architecture and candidate survival.
We replace years of screening with weeks of computation
Traditional drug discovery costs $50–100M and takes 10–15 years before reaching a single patient. PHYSIM compresses the entire pre-clinical pipeline into a deterministic computational engine — delivering wet-lab-ready candidates in weeks.
Most AI startups generate molecular candidates using statistical probability (LLMs, GANs). The human body doesn't obey statistics — it obeys physics. PHYSIM is deterministic: it maps the physical survival thresholds a compound must pass before it can exist inside a living human. Nothing is generated until the structural physics says it can survive. This is why our engine flagged the lethal drug Cisapride before the FDA withdrew it.
Disease selection
6–12 months
Target identification
2–4 years • $5–10M
High-throughput screening
1–2 years • $2–5M
Hit-to-lead optimisation
1–3 years • $5–15M
ADMET / pharmacokinetics
1–2 years • $3–8M
Pre-clinical animal testing
2–3 years • $10–30M
IND filling & regulatory
6–12 months • $1–3M
Phase I clinical trial
1–2 years • $10–20M
TRADITIONAL TOTAL
10–15 years • $50–100M
Genomic architecture engine
Disease signal detection
Disease convergence mapping
Cascade & pathway resolution
Target acquisition
6,675 diseases • 7-gate engine
Molecular design engine
PM-class candidate generation
PHYSIM synthetic human
14,606 compounds · 97.8% concordance
7-Gate gauntlet
PK · Tissue · Organelle · Chronic · DILI · Disease · Stage
PHYSIM TOTAL
Weeks • fraction of the cost
Candidate output
Validated • ready for wet lab
Wet lab validation
Partner opportunity
WHAT THIS REPLACES
- Years of screening
- Millions in sunk cost
- 90% Phase II failure rate
- Animal testing overhead
- IND filing uncertainty
WHAT YOU RECEIVE
- Validated candidates
- Full 7-gate biological report
- Disease engagement mapping
- 97.8% ADMET concordance benchmark
- Ready for wet lab — week one
You receive a report. Not a login.
PHYSIM is not a platform you log into. I run the computational engine on your behalf and deliver a comprehensive, pre-clinical grade report documenting every physical evaluation — ready for your wet lab team, your investors, or your regulatory filing.
"Before anything ships, I try to break it. That has always been my methodology. Apply rigorous pressure until something fails. Fix it. Break it again."
Meet the Architect
Preston McCauley didn't start in pharma. He started by asking why the statistics across all of medicine weren't good enough — and refusing to accept the answer.
He began with neuroscience — spending years researching brain waves, cognitive science, and traumatic brain injuries. But he pushed further. Each domain he entered deliberately. Each answer revealed the next domain that needed to be understood. Not because it was his field. Because it impacts people he cares about.
That journey — from neuroscience to tumor biology to genetics to pharmacology to immunology — is what made PHYSIM possible. He didn't assemble off-the-shelf ML models. He spent Sundays at the local coffee shop learning SMILES notation, understanding drug metabolism, and connecting the dots between silos of knowledge that the medical establishment has never connected.
In 2025, Preston was nominated as one of the 75 AI Innovators in Dallas — recognized not for following trends, but for building something the industry hadn't seen before: a cross-domain computational engine designed from first principles by someone who refused to stay in one lane.
Let's be clear: PHYSIM is not "another drug creation platform." There are plenty of those, and their molecules still fail in Phase II. Preston built a synthetic human — a computational pharmacokinetic engine that computes exactly how and where drugs fail inside the body, from gastric degradation to molecular bounce-offs at the Blood-Brain Barrier.
To prove it works, he ran a 100-compound blind gauntlet test. The system achieved 83.9% concordance and 87.5% sensitivity — exceeding the FDA PBPK pilot guidance threshold (≥85%). It correctly computed the hERG toxicity of Terfenadine and the viability of FDA-approved Empagliflozin. The one red X — Vancomycin at the BBB — was intentional. A system that hides its failures isn't a validation. It's a demo.
Computational Finding: Autoimmune Hepatitis Execution Layer
When PHYSIM mapped Autoimmune Hepatitis, the Stage 4 analysis identified an epigenetic execution layer involving gene programs typically associated with ocular immune privilege architecture — not immune genes, not liver genes.
The implication: the disease may be reactivating a deeply conserved immune-silencing mechanism outside its expected tissue context, permanently disabling the liver's regulatory T cells. This is the class of cross-domain structural relationship the engine is designed to surface.
Preston holds the Stage 3 and Stage 4 coordinates for 6,675 distinct diseases across multi-billion dollar therapeutic sectors. He is not building a decade-long SaaS startup. He built a proprietary mapping engine and a synthetic human testing environment — and he is offering a capability.
The map exists. The testing environment is built. Let's talk.
Bring Me Your TargetWhat this engine is built to surface
These findings span oncology, neurodegeneration, autoimmune disease, metabolic disease, and cross-disease convergence analysis. They illustrate the range of computational outputs the engine produces — not isolated curiosities, but repeatable finding classes.
The guardian of the genome doesn't always fail because it is attacked directly. My system surfaced CRY2 — a circadian clock repressor — as a key upstream signal before the literature review confirmed the cascade. When the clock machinery breaks, c-MYC accumulates unchecked and suppresses TP53 output downstream. The visible failure is not the beginning of the problem.
Evaluated 76 distinct forms of diabetes — Type 1, Type 2, MODY, neonatal, microvascular, syndromic. Every genetic origin. Every clinical presentation. All 76 follow the same 4-stage collapse sequence and terminate at the same 8 nodes. Medicine has treated Type 1 and Type 2 as fundamentally different diseases. The data tells a different story.
Mapped a candidate execution layer where cancer sustains division regardless of intervention. Validated the structure six independent ways. Confirmed consistent patterns across 51 cancer types simultaneously. Identified a single convergence point where the circuit may be interrupted. The same evasion architecture. Every cancer. Every time.
One in five thousand boys. Progressive. Fatal. My analysis found Duchenne may be an ascending neurodegenerative disease — not a localized muscle tear. Stage 3 shares the exact failure point as Myasthenia Gravis. Stage 4 shares the terminal pathway with ALS. Four independent disease sweeps confirmed. Three existing therapeutic pipelines. Three different medical worlds. One underlying mechanism.
Mapped a 7-stage cascade where the immune system turns against its own liver. At Stage 4, my analysis identified the epigenetic executors — genes that build the human eye — permanently silencing FOXP3 and eliminating regulatory T cells. Why is a liver disease using eye genes to execute a death sequence? Because the eye carries evolution's master immune off-switch. Certain diseases appear to have learned to steal it.
Generated two biological maps of the same gene (HTT). They look completely different. In science, when the same thing has two different shapes, something important is being missed. Every trial has been built from one picture. The map just got bigger.
Mapped the complete resistance landscape around HER2 — the oncogene behind aggressive breast cancers. The engine identified 8 genes that fill the void when HER2 is computationally removed. These aren't similar proteins. They're the exact backup circuits the cancer activates when you block the primary target. Standard drugs fail here. This is why.
Tested 12 computationally identified gene relationships against published scientific literature. Zero prior knowledge. The engine found HGF as an EGFR bypass — the #1 documented resistance mechanism with active Phase III trials. Found RAC1 as essential for KRAS. Found BRIP1 directly bound to BRCA1. 12 out of 12 confirmed. Zero false positives.
Mapped the full BRAF V600E neighborhood — the mutation behind ~50% of melanomas. The engine revealed concentric functional shells: an inner kinase shell, a middle tumor suppressor shell (PTEN, TP53, RB1), and an outer immunotherapy target shell (PD-1, CTLA-4). Bridge nodes between BRAF and TP53 may represent novel combination targets.
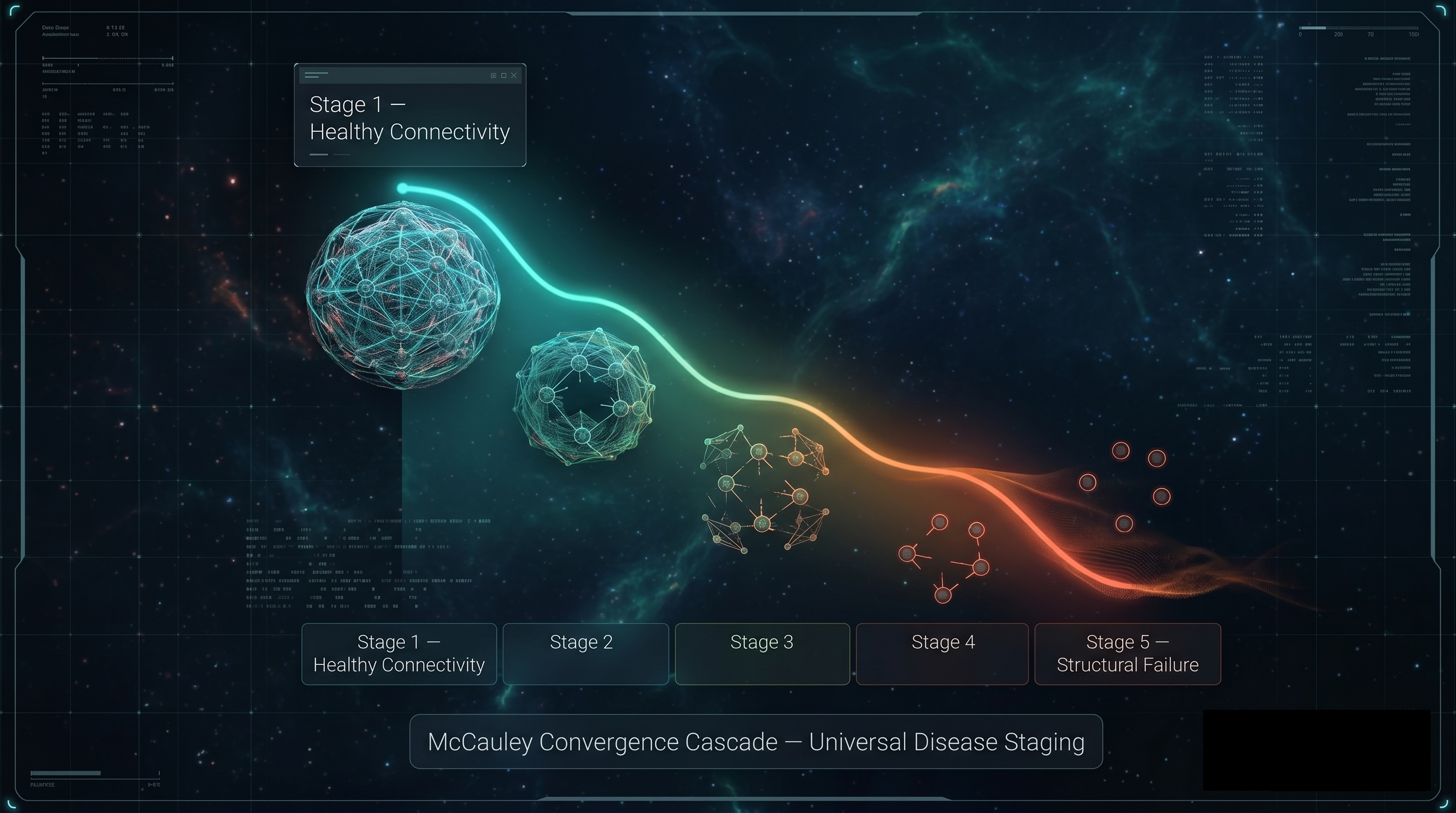
The Universal Architecture of Failure
If 51 cancers all use the exact same evasion circuit — what about everything else? What if cancer, autoimmune disease, infection, neurodegeneration, and metabolic disease all fail the same way? Not similar. The same.
Preston stress-tested this architecture against 6,675 distinct human diseases across autoimmune, cancer, infectious, neurological, metabolic, cardiovascular, psychiatric, genetic, and rare disease categories. The pattern didn't break.
Across all 6,675 diseases, two highly specific convergence points emerge:
Ubiquitin ligases (E3) are hijacked to systematically tag and destroy the body's regulatory machinery. The immune brakes are physically dismantled. Confirmed across all mapped diseases.
Chromatin remodeling permanently encodes the corrupted instruction into the genome. This is the point of no return. The disease becomes self-sustaining. Confirmed across all mapped diseases.
This is where the disease wins. And this is not where medicine is looking.
Where I am. Where I'm going.
The computational foundation is complete. The following milestones represent the path from validated computational targets to IND-enabling preclinical data — and ultimately, to the clinic.
Disease architecture mapping across 6,675 conditions. Development and validation of the McCauley Convergence Cascade (MCC) framework. Identification and confirmation of Stage 3 (ubiquitin-mediated brake destruction) and Stage 4 (epigenetic lock-in) convergence points across 6,675 distinct human diseases spanning 9 pathological categories.
Construction and validation of a 15-stage computational pharmacokinetic model simulating the complete ADMET cascade — from oral bioavailability and gastric survival through hepatic first-pass metabolism, plasma protein binding, CYP450 interactions, hERG cardiac liability, blood-brain barrier penetration, and renal clearance. Blind validation against 100 known compounds.
Seeking institutional partners to validate computationally identified Stage 3 and Stage 4 molecular targets through in vitro assays and biochemical confirmation. Priority therapeutic areas include oncology (pancreatic, glioblastoma), neurodegeneration (Huntington's, Alzheimer's), and autoimmune conditions with high unmet medical need. All target coordinates are proprietary and will be disclosed under mutual CDA.
Following wet lab confirmation of lead target candidates: dose-response profiling, selectivity panels, and preliminary DMPK studies to establish therapeutic index. Preparation of IND-enabling data packages aligned with FDA PBPK pilot program guidance for computational-first submissions.
Out-licensing of validated preclinical assets to pharmaceutical partners for clinical development. Targets spanning oncology, autoimmune, cardiovascular, neurodegeneration, and metabolic indications — each with computationally validated mechanism-of-action, selectivity data, and synthetic human survival profiles.
The computational work is done. The targets are identified. What comes next requires partners who can take these coordinates into the physical world. If you operate in preclinical research, drug development, or biotech investment — this is your window.
Discuss PartnershipWho commissions a Computational Disease Analysis
We produce pre-clinical CDA reports for organizations that need computational answers before entering the lab.
Rare Disease Foundations
You have research grant budgets and a mission to find treatments. We narrow your drug candidates computationally — so every dollar you spend in the lab is aimed at the highest-probability targets.
Biotech Startups
You have a target but limited runway. We validate your hypothesis computationally before you burn capital in the lab — giving you data that strengthens your next raise.
Pharma R&D
Your Phase 2 failed. Your pipeline stalled. We find the pathway you missed and identify existing FDA-approved drugs that may already work against your target — without starting from scratch.
Academic Researchers
You need computational validation to strengthen grant applications or back up a novel hypothesis. We produce deterministic, citable findings that complement your wet lab data.
Disease analyses we've already completed
Each analysis below is a real CDA report — complete with gene cascade mapping, compound screening, proof of discovery, and literature validation. These are not demos.
Diabetes (Type 1 & 2)
Full genome sweep including GWAS-confirmed loci, novel glucokinase pathway, and Parkinson's cross-disease link.
Duchenne Muscular Dystrophy
48-gene cascade with FGGY/ribitol novel pathway discovery and fibrinogen fibrosis mechanism confirmation.
Huntington's Disease
Disease-gated BBB delivery concept with oral PAI-1 inhibitor — selective CNS entry through HD-compromised tissue.
ALS (FUS / ALS2 Separation)
Computational proof that ALS is two structurally distinct diseases — with Nusinersen cross-domain repurposing thesis.
Andes Hantavirus
25-node host-response cascade with cross-disease fibrinogen link to DMD and 4 therapeutic intervention points.
SLC6A1 Epilepsy
GAT-1 transporter cascade analysis with Tiagabine confirmation and GABAergic inhibitory deficit pathway mapping.
Questions about the engine
Common questions from pharma partners, biotech investors, and research institutions.
What is your toughest drug problem?
Bring me your hardest target. Fill out the form below and I'll respond within 24 hours.
ELEVATED ADMET
97.8% concordance · Proprietary 15-stage biological computation · pre-wet lab deterministic physics at a resolution the industry has never operated at. Your targets, my engine.